The NIH Clinical Center used to commission artwork for some of their lectures. Here is one for “Phobias and Panic Disorder” from 1985.
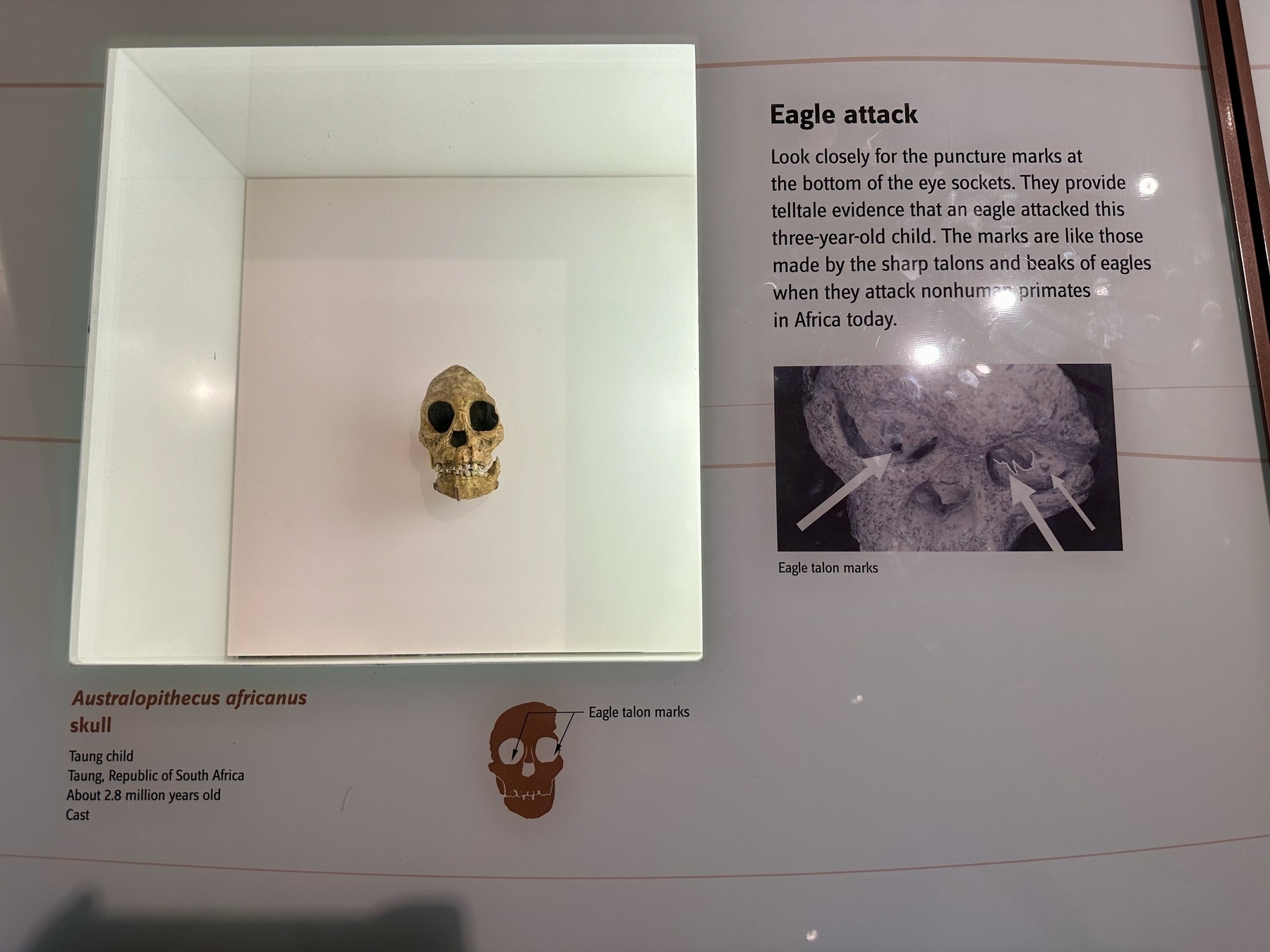
In retrospect, that friend worried about an eagle flying away with his toddler as prey wasn’t completely bonkers.
From the early humans exhibit at the National Museum of Natural History.
Derek Lowe writes about a recent Cancer Cell paper pitting glioblastoma cells against each other in a mouse model:
A single clonal line that hit on high Myc expression could outcompete fifteen thousand others from a standing start!
As someone who’s treated patients with Burkitt lymphoma, the Myc-dependent cancer, I can absolutely believe this.
From the archive: the author presenting some preclinical work on the cell cycle at the AACR annual meeting in Washington DC, circa 2017. Little did I know that six years later I’d be living just a few blocks down the street.
More crowded than usual.
For your (and mine, time permitting) weekend reading, listening, and/or viewing pleasure: the Tim Ferris interview with Nassim Taleb and Scott Patterson. I sure hope you are familiar with the former; the latter is a reporter for The Wall Street Journal who also wrote a book about “black swan traders”, which, yes, is probably going to the pile the antilibrary. It is a 2-hour discussion rightfully described as a feast.
September lectures of note
It’s been a while, but school is back in session and so are interesting online lectures. Here are a few I plan on attending, time permitting:
- Alpha Spending for Clinical Trials by Dr. James F. Troendle of NHLBI (Thursday, September 7, 3pm EDT)
- Varicella Zoster Virus in Glioma Etiology and Survival: Evidence of a Beneficial Virus? by Dr. Stephen Francis, UCSF (Tuesday, September 12, 2pm EDT)
- 2023 Judith H. Greenberg Early Career Investigator Lecture by Dr. Akhila Rajan, FHCC, and I know the title doesn’t tell you much but per the description “Dr. Akhila Rajan will discuss her research in a 30-minute talk on investigating how fat cells communicate with the brain, followed by a 30-minute live Q&A” (Wednesday, September 27, 1pm EDT)
One I absolutely must attend is held tomorrow (Thursday, September 7) at 6pm EDT, when I will talk about RNA cell therapy as the keynote speaker at the Maryland BioNetworking Summit, held at the BSE Facility at the Universities at Shady Grove in Rockville. It is in-person only and free to attend, if you register here.
Reading Adam Mastroianni’s latest article, about the vacuousness of psychology, and it looks like the world is ready for psychohistory. Now if only we had an intelligence greater than ours to develop it…
A few more notes on that vaccine study
Figures from the which-arm-for-the-second-shot study I wrote about yesterday reminded me of the delightfully titled “An illusion of predictability in scientific results: Even experts confuse inferential uncertainty and outcome variability” published in PNAS. [Note: ↬Dean Eckles ] To be clear, this is not the error study authors made, but see for yourself the chart that got them a USA Today head nod:
Spike-specific CD8 T-cells from Ziegler et al. eBioMedicine 2023.

So much variability! And even with 143 samples, still so much uncertainty. But increasing the sample size would help the variability much, as noted in PNAS:
Inferential uncertainty vs. outcome variability from Zhang et al. PNAS 2023.

You can squish the error bars, but you can’t squish your study population. Anyway, I thought it was interesting.
But now that we have that figure from the vaccine article up, let’s note two more things:
- The percentages in question are absolutely tiny. Median is 0.06% in the ipsilateral and <0.03% in the contralateral group, if we just eyeball it. At that point you are looking at what, 2–3 dots on the flow cytometry scatterplot? Interoperator variability must be huge.
- Their cutoff for saying that someone “has” spike-directed CD8 T cells was, I presume from the dotted horizontal line labeled “DL”, 0.03%. They based this off of historic values of unvaccinated healthy controls from this paper from the same group. I may be getting into the weeds too much here, but the text of that article says that “0.03% of reactive T cells was set as the detection limit based on the distribution of T cell frequencies after control stimulations”. This is so vague that it’s perfectly useless, but looking at Figure 1 gives it away: they picked one standard deviation away from the mean for the CD4-positive cells as the detection limit for both CD8-positive and CD4-positive spike-specific T cells. And even in that experiment, the variability of spike-specific CD8 T cells is so much greater than that of the CD4+ ones (0.02% versus >1% maximum in the healthy, unvaccinated and unexposed-to-SARS-CoV-2 controls). So they are not only extrapolating old experimental data into the new one, they are extrapolating one cell type into another when no such extrapolation should be made. Put hey, it came out in Nature Medicine, so it must be OK. Sigh.
Here's why.
There was something particularly irksome about a USA Today article from a few days ago — it prompted 3, count them, three tweets posts Xs from me — and I wanted to figure out what bothered me so. Here is the headline:
Left or right arm: Choosing where to get vaccinated matters, study suggests. Here’s why
No, it’s not the typography, although they should either not have had a full sentence in their headline, or else should have finished it with a full stop. But then they would have lost the chance for the click-baity Here’s why as a prelude to an article [Note: OK, this can get real confusing real fast since there are two articles I am writing about: the USA Today’s newspaper article, and the research article to which it refers. So, let’s use article for the newspaper, and manuscript for the research article. Because why not? ] about Real Science™ which — color me astonished — takes a hypothesis-generating study and presents the hypotheses it generated as the final results.
To its credit, the article starts of with a link to the manuscript and the name of the journal where it was published, which is eBioMedicine, part of the proliferating Lancet family, impact factor 11.1. [Note: Although, you know what they say about impact factors. ] Good! They also invited an independent researcher to comment. And I am sure that his comments were similar to mine, although of course most of what he said (or more likely wrote in an email) didn’t make it. What ended up on the page were two blurbs about precise vaccination from the director of a Precision Vaccines program. Gasp.
But these are all side attractions. The biggest problem is this: scientists want to compare people who had a two-dose vaccine shot in the same arm to those who had it in different arms; in the manuscript, these were called ipsilateral and contralateral groups. They aren’t randomizing people to one versus the other, [Note: What they describe as randomization isn’t really so, but that’s a rabbit hole we better not get into. ] but with these being generally healthy people, and with the participants not having a choice as to where they will get a vaccine, that is not too much of an issue. Then they ask them some questions about vaccine side effects and draw some blood. The questions are about side effects and the blood is to check for “the strength of the immune response”.
Note that they don’t say at the outset that the groups would be different, and how. Would the opposite arm have fewer side effects? Better immune response? If so, in what way? More antibody? Stronger antibody? A different subtype of antibody? Better or worse cellular immunity? Which cell (among dozens)? More cells, stronger cells, or different cells? Or maybe the same side would be better?
The beauty of hypothesis-generating research (for the researcher) is that it doesn’t matter. Whatever you get, you will get it published, sometimes in a double-digit impact factor publication. I’ve sat on many a lab meeting where things like this were proposed and always, always, the comment is that “the results will be interesting whatever they are”. And they are right! But you will not know — cannot know — whether the results you got are based on an underlying physiology, or occurred purely by chance. That is where confirmatory studies come in.
Neither the manuscript nor the article recognize this. Among the many things they looked at, the researchers found two things that were different between the two groups: those who had the vaccine in the same arm had “more” of a certain type of immune cell than the other, and the opposite-arm group had increased expression of a certain marker on yet another type of immune cell. “More” is in quotes because even that is more subjective than it appears — another rabbit hole — but even if true in this sample, it is at best a hypothesis that should lead to another, possibly smaller study, where you focus on these cells, with different operators counting them, and doing additional hypothesis-generating analyses on the side to figure out the why of it, which would lead into yet another confirmatory study… You get the idea.
This is not what the manuscript authors propose. Instead they take their result at face value and concoct a mechanism out of thin air that would explain the result. The journalist then takes the mechanism and presents it as the main research result, the Here’s why of that clickbait headline. There is a high bar for calling anything in science conclusive and the article does have the usual disclaimer that “more research and data is needed”. But the phrase has been repeated so much that it has lost all meaning, something you say to mark yourself as a “believer in science” while with a wink and a nudge you act as if the results were indisputable.
Fortunately, science is a strong-link problem: those who know what they are doing will adjust their beliefs accordingly, and down the line confirm or falsify these preliminary findings. Unfortunately, science doesn’t operate in a vacuum. If its covering of science is indicative, journalism, the fourth estate, is in a hole and digging deeper, taking others with them.
Not a day after his EconTalk episode, Adam Mastroianni wrote a most delightful essay about why people just can’t get each other: “Sorry, pal, this woo is irreducible”.
Well, most of it is delightful. The fifth paragraph is absolutely horrifying (you have been warned).