Emily Fridenmaker, who is a pulmonary disease and critical care physician, writes on X:
Everything is so complex.
Logging into things is complex, placing orders is complex, figuring out who to page is complex, getting notes sent to other doctors is complex, insurance is complex, etc etc. But we just keep doing it.
At what point is all this just too much to ask?
There are a few more posts in that thread, and I encourage you to read all of it to get a sampling of why doctors feel burnt out. Whether you are in medicine, science, or education, your professional interactions have slowly — They Live-style — been replaced by a series of fragile Rube Goldberg machines that worked great in the minds of their technocratic developers, but break, stutter, stammer, and grind to a halt as soon as they encounter another one of their brethren. Which is all the time!
Too much of our professional lives has been spent playing around with a series of Rube Goldberg nesting dolls,
[Note:
Before reading I Am a Strange Loop I would have apologized for mixing metaphors, but this is how our brains think and it doesn’t have to make sense in the physical world to be useful, so apology rescinded.
] 2FA inside a 2FA, and if Apple is wondering why people are taking more and more time to replace their aging iPhones, I bet a good chunk of them dread doing it because they don’t even know how many different authenticating services, email clients, education portals, virtual machines — and all other needless detritus sold to management by professional salespeople — they would need to log back into.
Don’t get me wrong: Rube Goldberg machines are fun to play with — The Incredible Machine was one of my first gaming memories — and they can even be useful for individual workflows. But mandating that others use your string-and-pulley concoction that will break at first unexpected interaction is sadistic. Just this Monday we had yet another AV failure at a weekly lecture held at a high-tech newly-opened campus. I knew there would be trouble the moment I saw that the only way to interact with any AV equipment was via a touchscreen that had no physical buttons and no way to remove the power cord, which was welded to the screen on one end, and went into a closed cabinet on the other. Lo and behold the trouble came not two weeks later: we couldn’t get past the screensaver logo. We ended up asking students to look at their own screens while guest lecturers were speaking — and nowadays everyone carries at least two screens with them to school — which was too bad, because I was looking forward to using the whiteboard which is as far from Rube Goldberg as it gets.
Me from 20 years ago would have salivated for that much technology in my everyday life, but I’m hoping it was a function of the time, not of my age, and that kids-these-days know better. My own kids’ experience with the great remote un-learning of 2020–2021 makes me hopeful that they will be more cautious about introducing technological complexity into their lives.
September 28, 2023
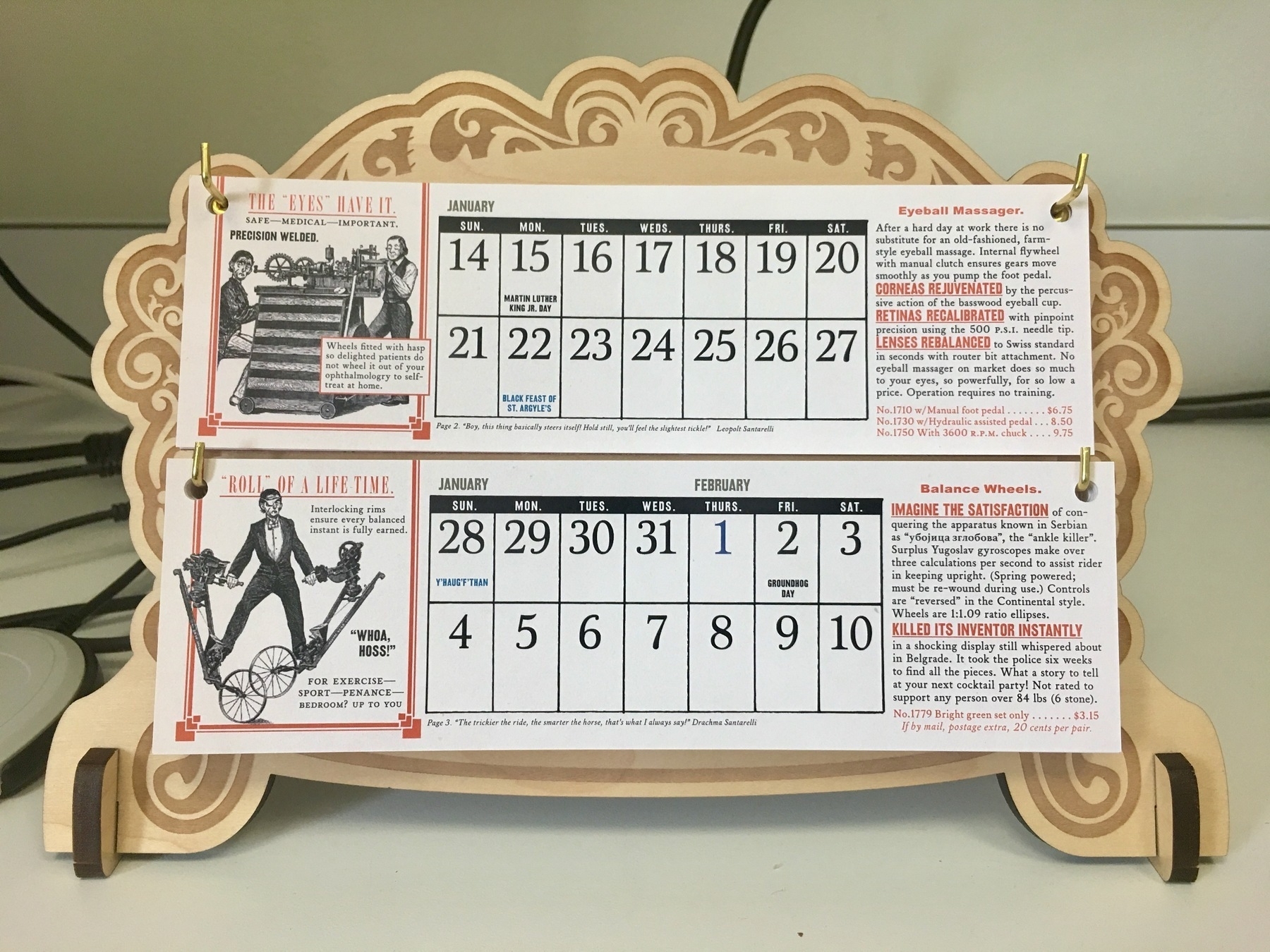
The Wondermark Calendar was great while it lasted. The 2018 edition had some strange ideas about what constituted a workout in Serbia.
The Wondermark Calendar for January 2018. Note the text on the bottom right.
📺 Next week is the season finale of Only Murders in the Building and I will have my one-paragraph review up then, but I’d like to note now that regardless of how they end up wrapping it up it has been the best season of TV in recent memory for the sheer joy of it. The soundtrackof all3 seasons makes for great tunes while at work, and the two Season 3 showsongs are now mandatory listening on our drive to school. So much better than The Afterparty, but then, I do prefer the East coast.
If there was any doubt whether I’m middle-aged,
[Note:
I am, in fact, past middle age, as I will turn 40 in December. The average life expectancy for a 39-year-old male in the United States is 37.85 years per the Social Security Administration actuary tables.
] the kids started school last month and it has been one back-in-my-day moment after another ever since.
This is the most recent one: the eldest has started 6th grade, which in the US is considered Middle School, and is apparently a big deal because that is when they start getting actual grades. Now, back in my day and — this is probably the more relevant fact — in Serbia, you started getting properly graded scored
[Note:
The unfortunate characteristic of the American school system is that it uses the term “grade” for too many distinct but adjacent concepts, so I will stick to “grade” for the yearly cohort of kids, and use “score” for the number they get on assignments and at the end of each year.
] in 1st grade: there was none of this descriptive assessment shenanigans. It was also probably the reason why the teachers were so interested in what your parents did for a living. But this is not a tirade against descriptive scoring; I had that moment 5 years ago at our first encounter with the 1st grade. The 6th grade b-i-m-d moment was that the scoring is performed nearly real-time, is viewable by both parents and children via an online portal, and — this is what got me — includes whether you:
wrote your full name instead of only the first name on a line that says just “Name”;
checked all of the boxes on an end-of-class exit form, regardless of whether you performed the tasks outlined next to those boxes;
turned in your field trip forms on time.
This is all incorporated into your Science class score. Science. Class. Score.
Now, if the main goal in your life as a scientist is to apply to as many NIH grants as possible and perhaps even win some of them, then yes, science is mostly about box-checking and meeting deadlines. But if you want to call these endeavors “science”, I encourage you to scroll through Adam Mastroianni’s newsletter Experimental History and check your beliefs against some persuasive evidence that science is, in fact, the complete opposite of checking boxes and worrying about the next deadline, and that part of the reason it is stagnating (well, some sciences more than others) and that younger generations are more interested in becoming influencers, content creators, crypto millionaires or whatnot is that they have this misshapen idea about what science actually is from the backwards way it is being presented to them.
With good intent, I should add! There absolutely should be a way to encourage tweens, teens, and adolescents to be more responsible and contentious and middle school is as good of an age to start as any. Heck, there is even a ready-made textbook for it. But call it “life skills”, call it “civics”, call it “behavior” if you will, as we did back in my day. Just please don’t call it Science.
Update: if you thought my quip about box-checking skills being important for NIH grants was facetious, here is the winner of the 2021 Nobel Prize for Medicine describing a recent desk rejection from the NIH for failing to properly format his references on a grant application. Quo vadis, scientia?
I love that Anne calls the very first draft of what writers write as “shitty first drafts”. I love it not because I write shitty first drafts and then better second drafts, but because I only write shitty first drafts, and then hit publish.
We are three weeks into our clinical trials course for the UMBC graduate program. This remark will surprise absolutely no one, but: it was refreshing to see a classroom full of attentive, engaged students, interrupting, asking questions, having a dialogue, others jumping in, etc. Alas, I cannot take any credit for the interactions, as we have guest lecturers on for most weeks.
Regardless, the course has reminded me about how absolutely wrong I was back in December 2019, when during a post-conference[Note:
The link is for the 2019 ASH Annual Meeting abstract book, ASH being the American Society of Hematology, and I am only now realizing that — in what could be described as our profession’s version of burning man, which is actually quite fitting for an organization called ASH — they tear down the conference website each year to make a new one. So, the 2019 version is no more, but here is one for the 65th annual meeting in December 2023 although if you go to the website after December 2023 I am sure it will point you to the 66th and beyond. I could have linked to the Internet Archive version of the website from 2019 instead — in fact, here you go — but why relinquish myself of the opportunity for that burning man’s ash pun?
] dinner I stood on my soapbox and wondered in amazing why we were still wasting our time meeting in person once per year like barbarians, when we could in fact be having continuous virtual conversations on Zoom. Timely spread of scientific information and all that.
Well, I have apologized — in person! — to everyone who had to suffer through my Orlando diatribe, because the last 3 years have shown that while video conferencing may rightfully replace most business calls and other transactional meetings, it is absolutely abysmal for education for all parties involved. And it’s not just that any kind of non-verbal communication is lost, it is that even spoken language is stilted, muted, suppressed. With the slide-up-front, speaker-in-the-corner layout that is so common for lectures, you may as well be pre-recording it. It makes absolutely no difference.
And, attending a few online lectures every month myself, it is hard to decide what is worse: having it be completely online and trading off the quality of the lecture for more opportunity for interaction, or watching a live/hybrid lecture and being completely shut out from the discussion (because the in-person attendees take priority when it comes time to ask questions, and rightfully so).
Even at the most basic practical level: technology failure with an online lecture means no lecture; technology failure in-person means, at worst, using the whiteboard and interacting more, which actually makes me wish for more technology to fail. And if you absolutely need to have the slides to make your points, just print them out for your own reference, and share them beforehand for the students to view on their own screens, of which they will have many.
After the last couple of weeks of in-person work, I have to say: Some things simply can’t be done as efficiently — or at all — unless done in person. The bandwidth of, and fidelity of, being in the same room — even, maybe especially, during breaks and downtime, but during work periods, too, of course — of being able to pass objects back and forth, to have zero latency in conversation between multiple people. To not fuss with connections or broken software (Zoom, a scourge of computing, abjectly terrible software (I prefer … Google Meet (!) by a mile)) or cameras that don’t allow for true eye contact — where everyone’s gaze is broken and off and distracted. To dispatch with all of those jittery half-measures of remote collaboration and swim in the warm waters of in-person mind-melding is a privilege for sure, and a gift.
Education is one of those types of work that can not easily be replicated online.
[Note:
AR/VR being a big and obvious caveat here, but that will take a while.
] For evidence, look no further than the persistence of the physical university campus despite the plethora of free and paid online options. Were it not for the in-person factor, the higher education equivalent of The New York Times would have gobbled up the market by now. I’ll know the tide has turned once Harvard and Yale — which would be my first proxies for the NYT and WaPo of higher ed — start investing more in their online offerings to the detriment of in-person experience.
Humans are represented by a mass of 70 kg and a radius of 50 cm (we assume sphericity), while whales are represented by a mass of 10^5 kg and a radius of 7m.